

Kris English, PhD
Professor Emeritus of Audiology
University of Akron
This article is posted as we near the three-year anniversary of George Floyd’s murder (May 25, 2020). In the US, this crime reignited the Black Lives Matter movement, as well as renewed support for the LGBTQ+ community, indigenous persons, and others experiencing injustice.
However, as often happens, momentous events lose their impact over time. Protest signs fade and attention is directed elsewhere … all the more reason to routinely recommit to cultural humility and equitable audiologic care.

Cultural humility includes treating others with dignity. Following is a discussion of relational dignity, and how it might be communicated in audiology appointments.
Dignity
The concept of dignity is both commonplace and difficult to define, apart from a generalized belief that “We know when we see it, and we know when we don’t see it.”1-3 There is at least general agreement that dignity is a human right,4-6 and is “attached to all human beings irrespective of any of their achievements” (p. 71).7
Jacobson8 describes this specific aspect of dignity as “dignity-in-self.” Another aspect, highly relevant to person-centered care, is known as “dignity-in-relation…[referring] to the ways in which respect and worth are conveyed through expression and recognition… a matter of action and interaction …” (p. 17)
Relational dignity is reciprocal and mutual: “I dignify you by recognizing your self-respect; by dignifying you, I also dignify myself…”(p. 16).8 When dignity is not acknowledged in either direction, trust breaks down.9
We are fully aware that not all humans are treated as though they have equal worth. However, we may not be aware of the many subtle breaches in relational dignity. Jacobson lists a continuum of 24 types of social violations of dignity, many of which are egregious (e.g., exploitation, assault) and would never be permitted in a clinic setting. But the “lesser” end of the continuum should give us pause: they include dismissal, disregard, and grouping.
Dismissal describes the experience of discounting a person’s knowledge, concerns, and feelings. “In health care settings, serious medical conditions go untreated because doctors and nurses dismiss their patients’ ability to recognize and report accurately when something is wrong” (p. 27)8, consistent with Dr. Susan Moore’s experience, reported after she passed away.
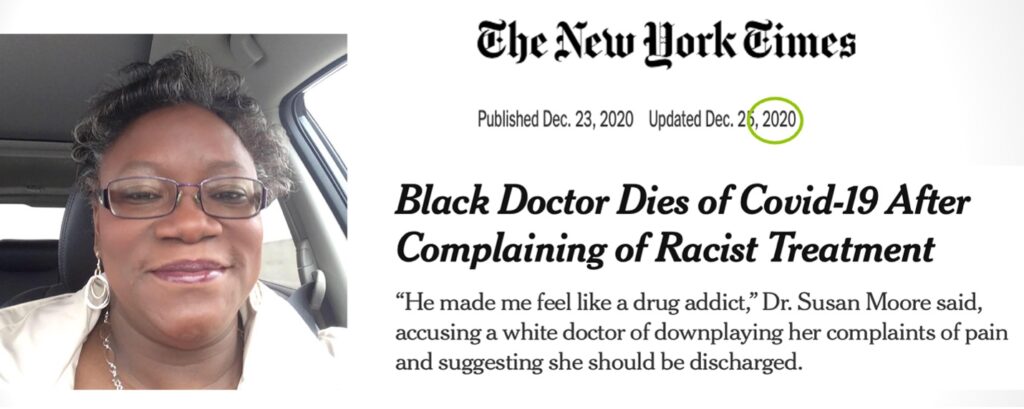
https://www.nytimes.com/2020/12/23/us/susan-moore-black-doctor-indiana.html
Disregard is behavior that communicates “I don’t believe you” when a patient reports concerns and needs. For example, a recent poll indicated that 60% of Black respondents reported higher rates of being disbelieved, and of being denied tests, treatments or pain medication they thought they needed.10 “Not being believed” has been a widely reported experience, much of it relating to the myth that Black individuals have a higher pain tolerance than Whites.11-14
Another breach, grouping, is one we already know how to define: “when people are seen and treated not as individuals, but only as indistinguishable and interchangeable parts of a unit” – a type of othering, the separation of “them” from “us.”
Needless to say, these kinds of dignity violations are not limited to Black patient experiences.15-17 As Jacobson18 points out: “Any human interaction can be a dignity encounter—an interaction in which dignity comes to the fore and is either violated or promoted” (p. 1538). Relevant to our commitment to cultural humility, equitable health care, and counseling applications, Jacobson poses this thought-provoking question: How can relational dignity be enacted in the design and delivery of healthcare?
Part 2 of this article will consider the Patient Dignity Question: “What do I need to know about you as a person to take the best care of you that I can?”

https://medium.com/@megansaxelby/dignity-a-framework-to-transform-school-culture-b50a7ace9ec7
References
- Dutra PEP, et al. (2022). Improving the perception of respect for and the dignity of inpatients: A systematic review. BMJ Open, 12:e059129.
- McClellan FM. (2020). Healthcare and human dignity: Law matters. New Jersey: Rutgers University Press.
- Schulman A. (2009). Bioethics and the question of human dignity. In B.T. Lanigan (Ed.), Human Dignity and Bioethics (pp. 3-13). Nova Science Publishers, Inc
- Baillie L, Matiti M. (2013). Dignity, equality and diversity: An exploration of how discriminatory behaviour of healthcare workers affects patient dignity. Diversity and Equality in Health and Care, 10, 5–12.
- Jones DA. (2015). Human dignity in health care: A virtue ethics approach. The New Bioethics, 21(1), 87–97.
- Miller, SC. (2017). Reconsidering dignity relationally. Ethics and Social Welfare, 11(2), 108-121.
- Nordenfelt L. (2004). The varieties of dignity. Health Care Analysis, 12(2), 69-81.
- Jacobson N. (2012). Dignity and health. Nashville: Vanderbilt University Press.
- Bazargan M, et al. (2021). Discrimination and medical mistrust in a racially and ethnically diverse sample of California adults. Annals of Family Medicine, 19(1), 4-15.
- Kaiser Family Foundation/Undefeated Survey on Race and Health. (2020). Race, health, and COVID-19: The views and experiences of Black Americans.
- Akinlade, O. (2020). Taking Black pain seriously. New England Journal of Medicine, e68(1-2).
- Hoffman KM, et al. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. PNAS, 113(6), 4296–4301.
- Schoenthaler A, Williams, N. (2022). Looking beneath the surface: Racial bias in the treatment and management of pain. JAMA Network Open, 5(6):e2216281.
- O’Connor MI. (2021). Equity360: Gender, Race, and Ethnicity: Why Don’t We Believe our patients? Clinical Orthopædics and Related Research, 479, 897-900
- Kamen CS, et al.(2019). “Treat us with dignity”: A qualitative study of the experiences and recommendations of lesbian, gay, bisexual, transgender, and queer (LGBTQ) patients with cancer. Support Care Cancer, 27, 2525–2532.
- Guadagnolo BA, et al. (2009). Medical mistrust and less satisfaction with health care among Native Americans presenting for cancer treatment. Journal for the Health Care of the Poor and Underserved, 20 (1), 210–226. doi.org/10.1353/hpu.0.0108
- Staats K, et al. (2020. )Dignity and loss of dignity: Experiences of older women living with incurable cancer at home, Health Care for Women International, 41(9), 1036-1058.
- Jacobson, N. (2009). Dignity violation in health care. Qualitative Health Research, 19(11), 1536-1547.