Kris English, PhD
Kris English, PhD
Professor Emeritus
The University Akron, Ohio US
Given: our counseling goal is to connect with and support each patient and their families. As we absorb their reports, our careful listening practices involve empathy, attention to nonverbal communication, and undivided attention.
Concern: when we respond, we may undermine our patient-centered intentions by using jargon, acronyms, and scientific terms – language that would not likely be understood by someone who is not a clinician.1 This communication problem has been widely observed, e.g., a recent study2 found that “Nearly 80% of [healthcare] appointments included at least one instance of unexplained jargon, with an average of more than four uses of jargon per visit” (p. 1262). Unclear communication is never our intent, especially when we learn how it can adversely affect patient outcomes.3-5
Communication habits learned early in our careers can be hard to recognize; e.g,, Watermeyer et al.6 noted in their study that “Despite reporting that they try to minimize the use of jargon, all of the audiologists used words and phrases such as ‘ototoxic effect, cochlea, low pitch, organ of hearing, mild to severe, sensorineural hearing loss’ with no further explanation to patients” (p. 760).
 Unconscious use of jargon has been dubbed jargon-oblivion. To help us sensitize ourselves to jargon, Pitt and Henderickson7 defined several categories, including Medicalized English, i.e., words which patients know but have a different meaning in the context of healthcare. A few audiology examples include frequency, threshold, and [speech] discrimination. In everyday English, what might these words mean to patients? Are there more examples?
Unconscious use of jargon has been dubbed jargon-oblivion. To help us sensitize ourselves to jargon, Pitt and Henderickson7 defined several categories, including Medicalized English, i.e., words which patients know but have a different meaning in the context of healthcare. A few audiology examples include frequency, threshold, and [speech] discrimination. In everyday English, what might these words mean to patients? Are there more examples?
Other categories include:
- Technical Terminology: words likely learned in grad school, e.g. disease names, acoustic measurements
- Alphabet Soup: acronyms, abbreviations
- Medical Vernacular: words not universally known or understood, e.g., anatomy, names of tests, test results
To help us break through jargon oblivion, we can review audiology terms commonly used in clinic and identify their categories. By filling in the attached table Jargon Oblivion Audiology Examples and discussing with colleagues, we take the first step in habit-breaking: awareness.
The Antidote: Plain Language
Plain language is a movement promoted in health systems defined as clear, succinct speech while mindfully avoiding verbosity, jargon, obscure slang and needless complexity.8 Intentional use of plain language and a gradual increase of scientific terms has been shown to support health literacy skills.9-11 More importantly, patients have indicated a clear preference for plain language: in a recent study, more than 90% of respondents preferred jargon-free language during healthcare encounters.12
Initial Challenges:
- Acknowledging the problem: Clinicians can sometimes struggle when it comes to using and adapting to spoken plain language with patients and care partners; some are unaware of this gap.13
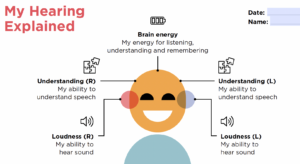
- Explaining our test results and recommendations with plain language. A starting point could be to revisit the impact of Ida Institute’s tool My Hearing Explained.14 It is appropriate for both children15 and adult patients.16,17
- Finding guidance: Although written materials are routinely analyzed for readability (e.g., SMOG: Simple Measure of Gobbledygook),18 there seems to be no correlate for verbal communication. Can we find a way to apply something like the SMOG framework to help us avoid jargon?
Obviously, plain language is most appropriate for first-time patients or patients who have not been tested recently. As the patient-audiologist relationship grows, “audiology speak” can be gradually introduced if the patient is interested.
Plain Language Habits Need Peer Group Support
Although posed in another context, Mantie et al.’s question “How can we change our habits if we don’t talk about them?”19 makes a valid point: we need to have ongoing discussions with colleagues about breaking jargon habits and using plain language as often as possible. Only our colleagues will understand what we want to achieve, and how to achieve it. It is up to the profession to work out what constitutes spoken “plain audiology language” toward the goal of communication that is understood the first time it is heard.20
References
- Smets EM et al.. (2026). The art and science of providing patients with helpful information.Patient Education and Counseling, 109514.
- Miller AN et al. (2022). Use of seven types of medical jargon by male and female primary care providers at a university health center.Patient Education and Counseling, 105(5), 1261-1267.
- Danaher TS et al. (2023). Improving how clinicians communicate with patients: An integrative review and framework. Journal of Service Research, 26(4), 493-510.
- Sciacca A et al. (2017). Exploring audiologists’ language and hearing aid uptake in initial rehabilitation appointments. American Journal of Audiology, 26(2), 110-118.
- Nair EL, Cienkowski KM. (2010). The impact of health literacy on patient understanding of counseling and education materials. International Journal of Audiology, 49, 71–75.
- Watermeyer J et al. (2015). Recall and understanding of feedback by adult patients following diagnostic audiological evaluation. International Journal of Audiology, 54(10), 758-763.
- Pitt MB, Hendrickson MA. Eradicating jargon-oblivion—A proposed classification system of medical jargon. J Gen Intern Med, 35, 1861–1864.
- Plain Language for Public Health. (n.d.)
- Grene M et al. (2017). Use of plain-language guidelines to promote health literacy. IEEE Transactions on Professional Communication, 60(4), 384-400.
- Yen RW et al. (2024). Clinician-spoken plain language in health care encounters: a qualitative analysis to assess measurable elements.Academic medicine, 99(6), 663-672.
- Peter M et al. (2024). Simplicity: Using the power of plain language to encourage patient-centered communication. Physical Therapy, 104(1), pzad103.
- Allen KA et al. (2023). Jargon be gone–patient preference in doctor communication.Journal of Patient Experience, 10, 1-5.
- Yen R et al. (2026). Measuring the use of spoken plain language by clinicians in healthcare encounters: a scoping review. Patient Education and Counseling, 109531.
- Ida Institute Archives. (n.d.) My Hearing Explained.
- Young J et al. (2025). My hearing explained for children: exploring use of this discussion tool in clinical practice. International Journal of Audiology, 64(4), 402-410.
- Nell LA et al. (2023). Satisfaction with hearing assessment feedback using the My Hearing Explained tool: client and audiologist perceptions.International Journal of Audiology, 62(5), 481-488.
- Lough M et al. (2025). The impact of using the Ida “My Hearing Explained” tool on audiologists’ language and patient understanding of hearing test results: A comparison with standard audiogram explanations. International Journal of Audiology, 64(5), 450-459.
- McLaughlin GH. (1969). SMOG grading – A new readability formula. Journal of Reading, 12, 639-646.
- Mantie R, Talbot BC. (2015). How can we change our habits if we don’t talk about them? Action, Criticism, and Theory for Music Education 14, 128-151.
- Warde F. et al. (2018). Plain language communication as a priority competency for medical professionals in a globalized world. Canadian Medical Education Journal, 9(2), e52.

 Notably, these items prompt clinicians to reflect on how the encounter was experienced from the patient’s point of view as well as our own. Responses that include often, very often, and almost always are consistent with person-centered and equitable care. Responses ranging from very rarely, rarely, or sometimes suggest that we should explore personal barriers, biases, or inhibitions and, if appropriate, consult with a colleague or mentor for support. If our responses are not aligned with our person-centered, equitable goals, Campbell et al.9 recommend “…a variety of implicit bias mitigation strategies named in the literature. These include continuous reflection on one’s beliefs on specific social groups, gaining access to regular training, and seeking feedback from outside sources such as the
Notably, these items prompt clinicians to reflect on how the encounter was experienced from the patient’s point of view as well as our own. Responses that include often, very often, and almost always are consistent with person-centered and equitable care. Responses ranging from very rarely, rarely, or sometimes suggest that we should explore personal barriers, biases, or inhibitions and, if appropriate, consult with a colleague or mentor for support. If our responses are not aligned with our person-centered, equitable goals, Campbell et al.9 recommend “…a variety of implicit bias mitigation strategies named in the literature. These include continuous reflection on one’s beliefs on specific social groups, gaining access to regular training, and seeking feedback from outside sources such as the  Why Belonging Matters: A Human Need that Impacts QOL
Why Belonging Matters: A Human Need that Impacts QOL ways to communicate to patients that they unquestionably fully belong.17,18 Communicating belongingness “entails an unwavering commitment to not simply tolerating and respecting difference (which is no small thing in a world of violent othering), but to ensure that all people are welcome and feel that they belong in the society with agency and not as provisional guests”(p. 160).4
ways to communicate to patients that they unquestionably fully belong.17,18 Communicating belongingness “entails an unwavering commitment to not simply tolerating and respecting difference (which is no small thing in a world of violent othering), but to ensure that all people are welcome and feel that they belong in the society with agency and not as provisional guests”(p. 160).4 The Barometer measures “belonging” in five contexts (family, friend, workplace, local, national) – none directly applicable to experiences in a healthcare setting but a potential research project.
The Barometer measures “belonging” in five contexts (family, friend, workplace, local, national) – none directly applicable to experiences in a healthcare setting but a potential research project. For inspiration, consider
For inspiration, consider  Kirsten Ellis, BA, MSc, RHAD, AssocFBSA
Kirsten Ellis, BA, MSc, RHAD, AssocFBSA
 When audiologists share relatable stories or connect patients with support groups, they help individuals see that they are not alone in their journey. For audiologists, recognising common humanity means acknowledging that perfection is unattainable. Mistakes happen and challenges arise in clinical practice. By fostering a culture where vulnerability is accepted, audiologists can support each other and their patients more effectively.
When audiologists share relatable stories or connect patients with support groups, they help individuals see that they are not alone in their journey. For audiologists, recognising common humanity means acknowledging that perfection is unattainable. Mistakes happen and challenges arise in clinical practice. By fostering a culture where vulnerability is accepted, audiologists can support each other and their patients more effectively. Kris English, PhD
Kris English, PhD


 Upskilling to an Essential Standard of Care
Upskilling to an Essential Standard of Care Taking the last question first: active listening is not about listening per se, but about interactivity. (It has been suggested that the term “conversational listening” might be more meaningful.1) While attending to a patient’s narrative, active listeners also verbally respond – with paraphrases, questions, affirmations, requests for clarifications, call-backs to previous topics – to assure patients that they are being heard.2,3
Taking the last question first: active listening is not about listening per se, but about interactivity. (It has been suggested that the term “conversational listening” might be more meaningful.1) While attending to a patient’s narrative, active listeners also verbally respond – with paraphrases, questions, affirmations, requests for clarifications, call-backs to previous topics – to assure patients that they are being heard.2,3

 Incongruence hinders our ability to communicate empathy and warm acceptance to persons associated with those biases, and efforts to do so come across as inauthentic.
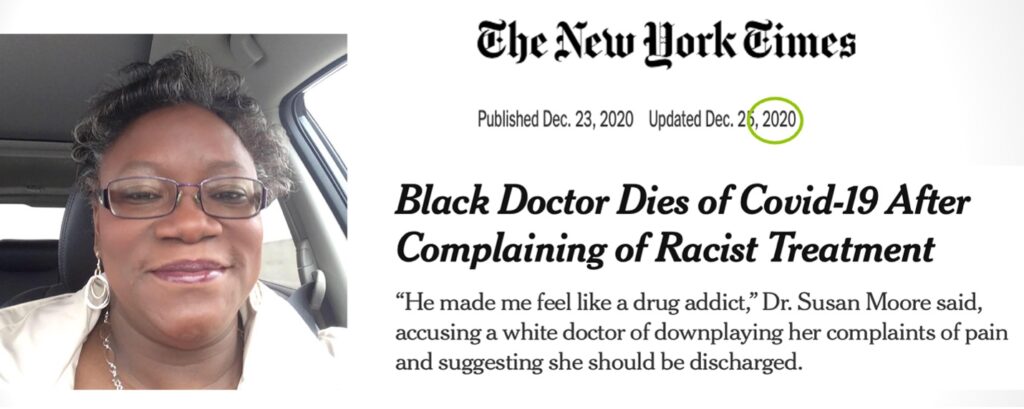
Incongruence hinders our ability to communicate empathy and warm acceptance to persons associated with those biases, and efforts to do so come across as inauthentic. It would not be unusual for helping professionals to miss the impact of unconscious / implicit bias on congruence – even Carl Rogers seemed to have overlooked it until rather late in his career. Crisp8 recently reported on two video recordings of Rogers’ therapy sessions with two different Black male patients, conducted 5 years apart. The first session from 1979 was described by peers as having a “therapist-centric perspective” (p. 223) with missed opportunities to respond with empathy to the client’s racism experiences and avoiding an exploration about their racial and cultural differences.
It would not be unusual for helping professionals to miss the impact of unconscious / implicit bias on congruence – even Carl Rogers seemed to have overlooked it until rather late in his career. Crisp8 recently reported on two video recordings of Rogers’ therapy sessions with two different Black male patients, conducted 5 years apart. The first session from 1979 was described by peers as having a “therapist-centric perspective” (p. 223) with missed opportunities to respond with empathy to the client’s racism experiences and avoiding an exploration about their racial and cultural differences.