

Audiologist
Southend University Hospital
NHS Foundation Trust
In Yoga, we are encouraged to minimise distractions. Now, I am speaking from a student’s point of view, as I certainly don’t possess the in-depth knowledge that my dear yoga teachers do. When laying in Savasana (the prone relaxation pose at the end of a class, and sometimes at the beginning) we are reminded that there are no distractions, there is nothing else we need to do at that moment apart from being present in the space. Often easier said than done!So to my surprise, when relaxing in Savasana one evening and listening to the teacher guide us through meditation, she reminded us that we were there for ourselves, we had no expectations on us at that time, and that this was a safe space for us to just “be.”
“Don’t bring your story.” – The Breakthrough
On hearing this my mind lit up (probably much to the disappointment of my yoga teacher) – how can this be carried over into our counselling? The clinical ego wants us to bring our “story” to each appointment. It tells us to reassure the patient that we know best, that our experiences and training (our story) are how we can best manage someone seeking help.
Additionally, in a more literal sense we don’t want to belittle our patients’ experiences by comparing them to our own. How often have we felt disheartened at being told “I know how you feel,” or “I’ve been though that, it’s not so bad”?
To truly listen, we shouldn’t bring our story to the appointment. By releasing our story and subsequent distractions, we can truly be present to listen.
The Yogi and the Clinician
My yogi has helped me work through what feels uncomfortable, or through a busy state of  mind to find peace in the present moment. When we are truly listening, are we also not working to find peace within ourselves to be fully present for the person in front of us?
mind to find peace in the present moment. When we are truly listening, are we also not working to find peace within ourselves to be fully present for the person in front of us?
I’ve often found myself in the midst of what I would feel is a difficult conversation, trying to push my clinical ego aside and allowing my patient to just talk. For me, this echoes working through what I feel is uncomfortable, allowing my patient to work through vulnerability to achieve a sense of calm (not necessarily a conclusion) in the appointment.
What are we doing to be self-aware, and how are we responding to this state?
To summarise my thoughts, I am reminded of a recent patient who attended for a review of his hearing aids. On the outside, one would assume he was a patient who could not hear well, felt his hearing had changed, and that an update was needed. However, once he came and took a seat, his body language communicated some further inner turmoil.
He confessed that he had been mishearing and forgetting important dates, the most  recent being his daughter’s landmark birthday celebration. I let him talk. With tears in his eyes, he told me that he had sought an appointment at his GP for an assessment for dementia. My clinical ego wanted me to reassure him, and tell him everything is fine and to push on with the appointment. But instead, we sat and explored his concerns. We asked each other questions and we sat through conversation and silences that were uncomfortable for the both of us. We came to an agreement that we would get his hearing aids as good as they can be for his dementia assessment, so that we can face things confidently with our heads held high.
recent being his daughter’s landmark birthday celebration. I let him talk. With tears in his eyes, he told me that he had sought an appointment at his GP for an assessment for dementia. My clinical ego wanted me to reassure him, and tell him everything is fine and to push on with the appointment. But instead, we sat and explored his concerns. We asked each other questions and we sat through conversation and silences that were uncomfortable for the both of us. We came to an agreement that we would get his hearing aids as good as they can be for his dementia assessment, so that we can face things confidently with our heads held high.
My general feelings once the appointment ended were that because of our interaction and agreement, we were both fully self-aware, in a compassionate environment that allowed for vulnerability (Hanson, 2009). Upon further reflection, I was struck by the parallels of Rogers’ (1961) three conditions of person-centered counselling: congruence with self, unconditional positive regard, and empathic understanding – all essential audiologic counselling skills. Of the three conditions, the foundational skill of self-awareness/congruence with self seems to generate almost no interest among audiologists.
So let’s start, shall we? Let’s develop a professional version of the prone relaxation pose Savasana – and breathe.

Reference
Hanson, J. (2009). Self-awareness revisited: Reconsidering a core value of the counseling profession. Journal of Counseling & Development, 87(2), 186-193.
Rogers, C. (1961). On becoming a person. Boston: Houghton Mifflin.




 A close reading of our ethics texts leads us to appreciate the ethical implications of listening (or not listening) to our patients. If we don’t fully absorb patient narratives, we are less likely to be “moved to action” toward personalized and comprehensive care. Promoting “close listening” (in the context of PCC) as an ethical practice warrants review and discussion within the profession.
A close reading of our ethics texts leads us to appreciate the ethical implications of listening (or not listening) to our patients. If we don’t fully absorb patient narratives, we are less likely to be “moved to action” toward personalized and comprehensive care. Promoting “close listening” (in the context of PCC) as an ethical practice warrants review and discussion within the profession.
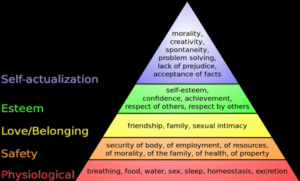 YES: Review Maslow’s Hierarchy of Needs
YES: Review Maslow’s Hierarchy of Needs
 Kris English, PhD
Kris English, PhD To manage the potential conflict between maintaining patient relationships and electronic records, let’s consider a relatively simple communication skill called signposting. The following definitions of signposting will resonate, since they are already routine practices in audiologic practice:
To manage the potential conflict between maintaining patient relationships and electronic records, let’s consider a relatively simple communication skill called signposting. The following definitions of signposting will resonate, since they are already routine practices in audiologic practice:
 This template assumes the clinician welcomes and supports SDM. Unfortunately, our available evidence suggests this assumption is not a given (e.g., Ekberg et al, 2015; Grenness et al., 2015). Our limited research has also only focused on decisions related to hearing aid acceptance and options. However, there are other SDM opportunities in an audiology appointment, and these could be easily overlooked.
This template assumes the clinician welcomes and supports SDM. Unfortunately, our available evidence suggests this assumption is not a given (e.g., Ekberg et al, 2015; Grenness et al., 2015). Our limited research has also only focused on decisions related to hearing aid acceptance and options. However, there are other SDM opportunities in an audiology appointment, and these could be easily overlooked. A student exercise: How do these comments differ? How might a patient respond/react to each, and why? What counseling/communication skills do you recognize? These essays provide some relevant background:
A student exercise: How do these comments differ? How might a patient respond/react to each, and why? What counseling/communication skills do you recognize? These essays provide some relevant background: David Luterman, D.Ed.
David Luterman, D.Ed.
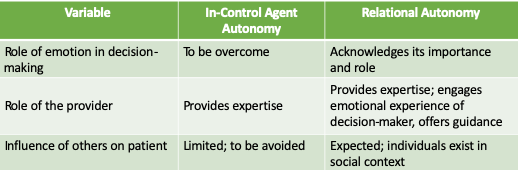
 In emotion based counseling, clients’ primary need is to be listened to non-judgmentally, not made to feel better. This is a hard concept for professionals to acquire, as our assumed mandate is to fix, and in the personal adjustment realm the fix is not apparent. Our clients are not emotionally disturbed; they are emotionally upset, which is appropriate to their life situation. The conventional response to someone who is upset is to try to make them feel better. The two favorite strategies are to instill hope (“Cochlear implants will make him normal”) or use positive comparisons (“It could be worse. He could have cancer, be deafer, etc.”).
In emotion based counseling, clients’ primary need is to be listened to non-judgmentally, not made to feel better. This is a hard concept for professionals to acquire, as our assumed mandate is to fix, and in the personal adjustment realm the fix is not apparent. Our clients are not emotionally disturbed; they are emotionally upset, which is appropriate to their life situation. The conventional response to someone who is upset is to try to make them feel better. The two favorite strategies are to instill hope (“Cochlear implants will make him normal”) or use positive comparisons (“It could be worse. He could have cancer, be deafer, etc.”).
 should we “go there?” We may think that talking about it will increase a patient’s self-stigma, yet if we don’t talk about it, we can be fairly sure it will not resolve on its own.
should we “go there?” We may think that talking about it will increase a patient’s self-stigma, yet if we don’t talk about it, we can be fairly sure it will not resolve on its own.