
reprinted with permission from ENT & Audiology, Sept-Oct 2025, 34(4).
 Kirsten Ellis, BA, MSc, RHAD, AssocFBSA
Kirsten Ellis, BA, MSc, RHAD, AssocFBSA
Hearing Aid Audiologist
The Hearing Care Partnership (South West), UK
Vulnerability, as defined by Brené Brown, is “uncertainty, risk, and emotional exposure” [1]. In audiology, patients often find themselves in vulnerable positions – whether it be acknowledging their hearing difficulties, accepting the need for hearing aids or dealing with the emotional impact of auditory changes. This sense of vulnerability can lead to feelings of shame, fear or frustration, making it difficult for patients to engage fully in their care.
From a professional standpoint, audiologists also experience vulnerability. They must navigate complex patient emotions, provide difficult diagnoses and manage expectations, all while maintaining their own emotional wellbeing. Recognising and addressing these vulnerabilities can foster stronger, more empathetic connections between patients and practitioners.
The Role of Shame and Courage in Audiological Care
Brené Brown’s research highlights the role of shame in preventing individuals from seeking help or accepting necessary changes. She explains that “shame corrodes the very part of us that believes we are capable of change” [2]. Many individuals with hearing loss delay seeking audiological care due to stigma, societal perceptions or personal fears about ageing and dependence. This shame can lead to denial, social withdrawal and a reduced quality of life.
Audiologists play a crucial role in dismantling these barriers by fostering an environment of courage and trust. Encouraging open discussions about hearing loss, normalising the use of assistive devices and validating patients’ emotions can empower them to embrace change rather than resist it. By incorporating vulnerability into practice, audiologists can shift the narrative from one of deficiency to one of adaptation and resilience.
Self-Compassion as a Tool for Patients and Practitioners
Dr Kristin Neff’s concept of self-compassion provides a powerful framework for addressing vulnerability in audiological care. Neff defines self-compassion as the ability to be kind to oneself in moments of suffering, rather than engaging in self-judgment [3]. Her three core elements of self-compassion – self-kindness, common humanity and mindfulness – are particularly relevant in audiology:
- Self-kindness over self-criticism. Patients often blame themselves for their hearing loss, feeling as though they have failed in some way. This can be especially true for individuals with noise-induced hearing loss or those who have avoided seeking treatment. Encouraging patients to practice self-kindness, rather than self-criticism, can help them approach their hearing health with a sense of care rather than guilt.
Audiologists, too, benefit from self-kindness. The field of audiology, like many healthcare professions, can be emotionally taxing. Self-compassion allows practitioners to acknowledge their limitations without feeling inadequate. When audiologists extend compassion to themselves, they are better equipped to provide compassionate care to others.
- Common humanity over isolation
Hearing loss can feel isolating, both socially and emotionally. Patients may feel that they are alone in their struggles, leading to withdrawal from social interactions. Neff’s principle of common humanity emphasises that suffering is a universal human experience.
 When audiologists share relatable stories or connect patients with support groups, they help individuals see that they are not alone in their journey. For audiologists, recognising common humanity means acknowledging that perfection is unattainable. Mistakes happen and challenges arise in clinical practice. By fostering a culture where vulnerability is accepted, audiologists can support each other and their patients more effectively.
When audiologists share relatable stories or connect patients with support groups, they help individuals see that they are not alone in their journey. For audiologists, recognising common humanity means acknowledging that perfection is unattainable. Mistakes happen and challenges arise in clinical practice. By fostering a culture where vulnerability is accepted, audiologists can support each other and their patients more effectively.
- Mindfulness over over-identification
Mindfulness involves being present with one’s experiences without excessive identification with them. Patients who over-identify with their hearing loss may see it as a defining characteristic, which can lead to frustration or despair. Mindfulness encourages patients to acknowledge their experiences without becoming overwhelmed by them.
In practice, audiologists can integrate mindfulness techniques by encouraging patients to engage with their hearing challenges in a non-judgmental way. Mindfulness-based listening exercises, for example, can help patients adjust to hearing aids or tinnitus management strategies with greater ease.
Creating a Culture of Vulnerability in Audiology
Embracing vulnerability in audiological care requires a cultural shift within the field. This can be achieved through:
- Empathetic communication – Practitioners should actively listen to patients’ concerns, validate their emotions and create a safe space for dialogue.
- Educational initiatives – Providing patients with information about the psychological impact of hearing loss can help normalise their feelings and reduce stigma.
- Support systems – Encouraging peer support groups or audiology counselling services can help patients feel less alone in their experiences.
- Self-compassion training for audiologists – Offering professional development focused on self-compassion and emotional resilience can benefit practitioners’ wellbeing and enhance patient care.

Conclusion
Vulnerability is an inherent aspect of audiological care, affecting both patients and practitioners alike. By applying the insights of Brené Brown on vulnerability and shame, and Kristin Neff on self-compassion, audiologists can create an environment where patients feel supported and empowered in their hearing health journey. Ultimately, embracing vulnerability in audiological practice fosters deeper connections, promotes healing and enhances the overall quality of care.
References
1. Brown B. Daring Greatly: How the Courage to Be Vulnerable Transforms the Way We Live, Love, Parent, and Lead. Gotham Books; 2012.
2. Brown B. The Gifts of Imperfection: Let Go of Who You Think You’re Supposed to Be and Embrace Who You Are. Hazelden Publishing; 2010.
3. Neff K. Self-Compassion: Stop Beating Yourself Up and Leave Insecurity Behind. HarperCollins; 2011.
 Abi Nardi
Abi Nardi
 We sat down… no one spoke for a minute, we just looked at each other, waiting for the other to speak…when suddenly he said to me: “ How comfortable I have felt for a moment, where nobody told me what to do or how, just waited for me to decide to speak…Now I´m going to tell you…”, Then I asked a few questions, since my patient described himself without questionnaires. And I asked myself: profound hearing loss? Without any testing? It turned out to be a patient with a wrong diagnosis.
We sat down… no one spoke for a minute, we just looked at each other, waiting for the other to speak…when suddenly he said to me: “ How comfortable I have felt for a moment, where nobody told me what to do or how, just waited for me to decide to speak…Now I´m going to tell you…”, Then I asked a few questions, since my patient described himself without questionnaires. And I asked myself: profound hearing loss? Without any testing? It turned out to be a patient with a wrong diagnosis. Luego de saludarnos, nos sentamos… nadie habló por un minuto, solo nos miramos, esperando uno al otro para que hablara… cuando de repente me dijo: “qué a gusto me he sentido por un momento, donde nadie me dijo qué hacer ni cómo, solo me espero a que me decidiera a hablar… Ahora te voy a contar…”, luego realicé pocas preguntas, ya que mi paciente se describió solo sin necesidad de cuestionarios. Y me pregunté: ¿Hipoacusia profunda? Sin haberle realizado siquiera un estudio. Resulto ser un paciente con diagnóstico equivocado desde su narración hasta las pruebas realizadas posteriormente.
Luego de saludarnos, nos sentamos… nadie habló por un minuto, solo nos miramos, esperando uno al otro para que hablara… cuando de repente me dijo: “qué a gusto me he sentido por un momento, donde nadie me dijo qué hacer ni cómo, solo me espero a que me decidiera a hablar… Ahora te voy a contar…”, luego realicé pocas preguntas, ya que mi paciente se describió solo sin necesidad de cuestionarios. Y me pregunté: ¿Hipoacusia profunda? Sin haberle realizado siquiera un estudio. Resulto ser un paciente con diagnóstico equivocado desde su narración hasta las pruebas realizadas posteriormente.
 mind to find peace in the present moment. When we are truly listening, are we also not working to find peace within ourselves to be fully present for the person in front of us?
mind to find peace in the present moment. When we are truly listening, are we also not working to find peace within ourselves to be fully present for the person in front of us? recent being his daughter’s landmark birthday celebration. I let him talk. With tears in his eyes, he told me that he had sought an appointment at his GP for an assessment for dementia. My clinical ego wanted me to reassure him, and tell him everything is fine and to push on with the appointment. But instead, we sat and explored his concerns. We asked each other questions and we sat through conversation and silences that were uncomfortable for the both of us. We came to an agreement that we would get his hearing aids as good as they can be for his dementia assessment, so that we can face things confidently with our heads held high.
recent being his daughter’s landmark birthday celebration. I let him talk. With tears in his eyes, he told me that he had sought an appointment at his GP for an assessment for dementia. My clinical ego wanted me to reassure him, and tell him everything is fine and to push on with the appointment. But instead, we sat and explored his concerns. We asked each other questions and we sat through conversation and silences that were uncomfortable for the both of us. We came to an agreement that we would get his hearing aids as good as they can be for his dementia assessment, so that we can face things confidently with our heads held high.

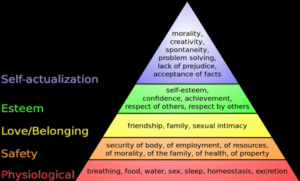 YES: Review Maslow’s Hierarchy of Needs
YES: Review Maslow’s Hierarchy of Needs
 Paul Peryman, MA, Dipl Aud (Melb), MNZAS-CCC, Audiologist
Paul Peryman, MA, Dipl Aud (Melb), MNZAS-CCC, Audiologist



 Diana Harbor, BA
Diana Harbor, BA Yesterday I had the privilege of being with a group of teenagers all living with hearing loss, using different technology from cochlear implants to bone implanted devices with different personalities and experiences of the world, some who had never met each other before. We all took part in an exciting improv, drama workshop at the Ear Foundation. Much of the afternoon was spent in small groups creating wonderful stories and weaving a single idea into a feast of creativity that JK Rowlings would have drooled at. And the real magic happened as Loydie, a DJ from Capital radio, revealed to us very simple techniques for keeping ideas going, for turning problems into new ideas and for getting the best out of each other. The power of using the phrase “…yes and” and how to do this while listening and maintaining eye contact.
Yesterday I had the privilege of being with a group of teenagers all living with hearing loss, using different technology from cochlear implants to bone implanted devices with different personalities and experiences of the world, some who had never met each other before. We all took part in an exciting improv, drama workshop at the Ear Foundation. Much of the afternoon was spent in small groups creating wonderful stories and weaving a single idea into a feast of creativity that JK Rowlings would have drooled at. And the real magic happened as Loydie, a DJ from Capital radio, revealed to us very simple techniques for keeping ideas going, for turning problems into new ideas and for getting the best out of each other. The power of using the phrase “…yes and” and how to do this while listening and maintaining eye contact.

 Jeanine Doherty, Au.D., M.Phil., M.B.S, B.Soc.Sci.(Hons.),
Jeanine Doherty, Au.D., M.Phil., M.B.S, B.Soc.Sci.(Hons.),  As we know, ethics, legality and morality are each different, though related, constructs. Something can be legal, yet immoral to an individual, as our values lead to our personal morals. Moral distress arises when clinicians are unable to act according to their moral judgement and their Profession’s Ethical Code (Rodney, 2017). This distress is located not only within individuals when their actions mismatch their values, but also from within the broader healthcare structures of the clinician’s workplace. The socio-political structures that can create moral/ethical distress have been studied mostly within nursing, but the relevance of the concept to audiology should not be ignored. Moral distress also emerges from situations that are against all the principles of PCC.
As we know, ethics, legality and morality are each different, though related, constructs. Something can be legal, yet immoral to an individual, as our values lead to our personal morals. Moral distress arises when clinicians are unable to act according to their moral judgement and their Profession’s Ethical Code (Rodney, 2017). This distress is located not only within individuals when their actions mismatch their values, but also from within the broader healthcare structures of the clinician’s workplace. The socio-political structures that can create moral/ethical distress have been studied mostly within nursing, but the relevance of the concept to audiology should not be ignored. Moral distress also emerges from situations that are against all the principles of PCC. Harris and Griffin (2015) write that some organisational policies can lead to diminished care quality and cynicism with lack of teamwork and lower morale amongst clinical staff. In such a work-place, increased competition and mistrust develops between staff, while middle management level finds itself stuck between demands from higher-up levels (e.g. profit/cost outcomes) and the lack of teamwork and lower morale of the clinicians who are in moral distress. The physiological and psychological effects caused by the existence of moral distress can lead to burn-out, and then the staff member becomes ill, finds another better workplace, or just gives in, morally disengages, and carries on in a manner that is opposed to their values/morals (Musto, Rodney & Vanderheide, 2015). Lachman’s (2016) list of symptoms of burnout includes fatigue, general illness, headaches, insomnia, disillusionment, anger, negative self-concept and a loss of concern for others.
Harris and Griffin (2015) write that some organisational policies can lead to diminished care quality and cynicism with lack of teamwork and lower morale amongst clinical staff. In such a work-place, increased competition and mistrust develops between staff, while middle management level finds itself stuck between demands from higher-up levels (e.g. profit/cost outcomes) and the lack of teamwork and lower morale of the clinicians who are in moral distress. The physiological and psychological effects caused by the existence of moral distress can lead to burn-out, and then the staff member becomes ill, finds another better workplace, or just gives in, morally disengages, and carries on in a manner that is opposed to their values/morals (Musto, Rodney & Vanderheide, 2015). Lachman’s (2016) list of symptoms of burnout includes fatigue, general illness, headaches, insomnia, disillusionment, anger, negative self-concept and a loss of concern for others. Laya Poost-Foroosh, PhD., MClSc.
Laya Poost-Foroosh, PhD., MClSc.


