
 Kris English, PhD
Kris English, PhD
The University of Akron/NOAC
Audiologic counseling has many facets, including patient education (Clark & English, 2014). Patient education is not inherently easy: every audiologist has had those moments when we realize our patient doesn’t understand us. Sometimes the patient is emotionally distraught and cannot concentrate, and sometimes we unintentionally provide more information than the patient-as-learner can process.
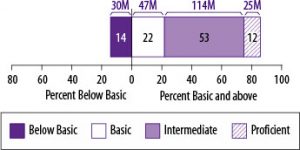
Another variable to consider is the patient’s health literacy. In addition to reading abilities, health literacy as measured by the National Assessment of Adult Literacy (NAAL)(2006) includes the ability to interpret graphs, do basic calculations (numeracy skills), and use a computer. We cannot take any patient’s health literacy for granted; in fact, the NAAL reports that more than 1/3 of adults in the United States (77 million) have limited (basic and below basic) health literacy skills (see figure below). Persons at basic/below basic literacy levels are not able to read or fully understand a newspaper article, fill out forms for Social Security, Medicaid or Medicare, or follow a bus schedule or calendar (Weiss, 2007). Relatedly, low health literacy is linked to more mistakes in medication usage, more emergency room visits and hospitalizations, and a higher risk of death. Relevant to audiology, it could mean misunderstanding instructions for hearing aid use, misinterpreting Internet sites about cochlear implant candidacy or auditory processing problems, or an inability to complete scales/questionnaires or provide a medical history.
Source: National Assessment of Adult Literacy
Health literacy skills are affected by age, education, income, health insurance status, and first language acquisition. But as Weiss (2007) warns us, “You can’t tell by looking” (p. 16).
Health literacy is a topic of high interest these days because health-related information continues to grow in complexity. This article has two parts: defining health literacy, and suggestions for audiologists on how to address health literacy concerns in their patient care.
Definitions of Health Literacy are Evolving
The definitions of health literacy have evolved rather quickly, from the static “snapshot” described in the figure above, to a dynamic process of growth and empowerment (Nutbeam, 2008). For instance, rather than pinning down health literacy as an unchangeable state as the NAAL data might imply, Zarcadoolas et al. (2005) prefer to define health literacy as “the wide range of skills, and competencies that people develop to seek out, comprehend, evaluate and use health information” (emphasis added)(p. 196). Such development can occur independently on the patient’s end, but it also can occur as a result of effective communication with health care providers. In other words, if we counsel and educate effectively, a patient’s health literacy level should increase over time.
Berkman et al. (2010) list several definitions of health literacy, but their own refinement is most suitable for our purposes:
Health literacy is the degree to which individuals can obtain, process, understand, and communicate about health-related information needed to make informed health decisions (p. 16)
They added the phrase “communicate about” to the Institute of Medicine’s 2004 definition because they considered oral communication skills (listening and speaking) to be a critical part of health care – as do audiologists and others. For instance, Ishikawa and Yabo (2008) point out that, in addition to NAAL’s consideration of functional skills (reading, interpreting graphs, computation, computer use), communication skills are also essential, including the ability to:
- Articulate health concerns
- Describe symptoms accurately
- Ask pertinent questions
- Understand verbal information accurately
Another dimension to health literacy is media literacy, or the ability to critically evaluate media messages in all formats. Additionally, health literacy is affected by context: patients may be proficient in managing medications and appointments for other health conditions, but with no prior experience with hearing loss, they may not immediately be ready to apply what they know to the novel context of audiologic care. And although not mentioned in the health literacy literature, audiologists might want to add understanding/use of technology (apart from computers) as a health literacy skill.
Applications for Audiologists Continue reading
![photo[1]](https://advancingaudcounseling.com/wp-content/uploads/2016/05/photo1-300x300.jpg) Nicolle Yopa, Class of 2015
Nicolle Yopa, Class of 2015 because John had class. We told her we had planned on an hour because many important things needed to be discussed; regardless, they opted to cut the appointment short so that John could make the last 20 minutes of class. My supervisor reluctantly agreed to let John leave with the hearing aids and have his parents practice with him at home.
because John had class. We told her we had planned on an hour because many important things needed to be discussed; regardless, they opted to cut the appointment short so that John could make the last 20 minutes of class. My supervisor reluctantly agreed to let John leave with the hearing aids and have his parents practice with him at home. Alison Marinelli, Class of 2018 (AuD/PhD)
Alison Marinelli, Class of 2018 (AuD/PhD)

 John Greer Clark, PhD
John Greer Clark, PhD But not all patients who come through our doors have reconciled themselves with their hearing loss. Some still harbor varying degrees of denial, continuing to place much of the blame for communication failures on the speaking habits of others. And these others continue to be viewed as residing in the enemy camp, pushing for actions that are not wanted or that are not perceived as needed.
But not all patients who come through our doors have reconciled themselves with their hearing loss. Some still harbor varying degrees of denial, continuing to place much of the blame for communication failures on the speaking habits of others. And these others continue to be viewed as residing in the enemy camp, pushing for actions that are not wanted or that are not perceived as needed. Kerri Hudson, AuD
Kerri Hudson, AuD
 Emily Pajevic, Class of 2015
Emily Pajevic, Class of 2015 How does an audiologist best serve Amanda and other adolescent patients? We cannot continue to primarily address the parents, undermining the patient’s knowledge and concern for his/her own healthcare and yet cannot ignore the parent’s need for understanding and the crucial role that they play. In healthcare, as well as our own profession, this topic of interacting with adolescents needs to be explored. If the unknown prevents us from providing the best care to this patient population, it is time to delve into this uncharted area, further expanding our knowledge and understanding to enhance our field and our impact on those we serve.
How does an audiologist best serve Amanda and other adolescent patients? We cannot continue to primarily address the parents, undermining the patient’s knowledge and concern for his/her own healthcare and yet cannot ignore the parent’s need for understanding and the crucial role that they play. In healthcare, as well as our own profession, this topic of interacting with adolescents needs to be explored. If the unknown prevents us from providing the best care to this patient population, it is time to delve into this uncharted area, further expanding our knowledge and understanding to enhance our field and our impact on those we serve. 
 Michael Squires, Class of 2014
Michael Squires, Class of 2014 What went wrong? It is obvious that this appointment had come to a point where an audiologist was no longer able to help. Unfortunately, this patient was never referred to anyone who could. There are many instances when a patient in an audiological setting should be referred to another professional for further examination. However, there is one such instance that is consistently ignored; depression. It seems intuitive that any major life changes, including learning of one’s hearing loss, has the potential to cause symptoms of depression. Audiologists are many times the first to notice depression and stress caused or exacerbated by a hearing loss. Yet, when these signs are noticed, whether they are caused by news of a hearing loss or some other event, what is the next step for an audiologist? According to the American Academy of Audiology’s Code of Ethics:
What went wrong? It is obvious that this appointment had come to a point where an audiologist was no longer able to help. Unfortunately, this patient was never referred to anyone who could. There are many instances when a patient in an audiological setting should be referred to another professional for further examination. However, there is one such instance that is consistently ignored; depression. It seems intuitive that any major life changes, including learning of one’s hearing loss, has the potential to cause symptoms of depression. Audiologists are many times the first to notice depression and stress caused or exacerbated by a hearing loss. Yet, when these signs are noticed, whether they are caused by news of a hearing loss or some other event, what is the next step for an audiologist? According to the American Academy of Audiology’s Code of Ethics: