Kris English, PhD
Kris English, PhD
Professor Emeritus, Audiology
The University of Akron
In early February 2023, the Ida Institute in Denmark announced that it is “significantly scaling back activities” as its funding comes to an end. Fortunately, its deep library of tools, online courses and other resources will remain available. These developments are highlighted here to honor Ida’s direct and enduring impact on audiologic counseling.
An Easy-to-Miss “Ida Impact:” A Consistent Focus on Person-Centeredness
Because of the many contributions Ida has made to audiologic practices in the past 15 years, its philosophical commitment to the concept of person-centered care could be taken for granted. When the organization began to define itself in 2007, the term had not been widely used; just 6 years prior, the Institute of Medicine’s (2001) report identified the concept of patient-centered care as a pillar of quality health care. Because of IOM’s stature, “PCC” became a widely accepted concept. Soon, however, concerns were raised about the term’s inherent limitations (e.g, Clarke & Fawcett, 2016; Mezzich et al, 2010; Miles & Mezzich, 2011). By listening carefully to those concerns as expressed by persons and families living with hearing loss and by thought leaders in audiology, Ida became one of the early adopters of another version of “PCC:” the more empowering concept of person-centered care.
The difference in wording may not have been immediately appreciated, but over time it began to sink in: the shift from patient to person reflects a difference in power, focus, and priorities. Compare these distinctions (Eklund et al., 2019):

- as defined by clinicians
- determined by test results (words, sentences in quiet, noise, etc)
- to address listening challenges at home, work.
Whereas … the focus of Person-Centered Care is to support a meaningful life…
- as defined by individuals with hearing loss and family
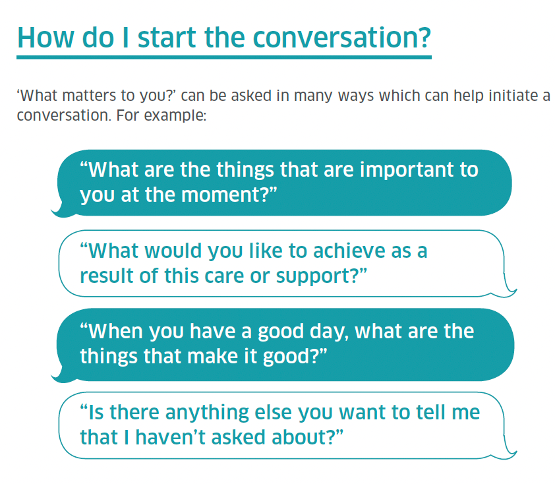
- determined by understanding the whole person (“what matters to you?”)
- whose individual goals may change over time.

Implications: Checking Our Priorities
These two models of centeredness represent different priorities, which by definition means assigning more weight or importance to one “thing” than to other things. For instance, clinician trainees understandably prioritize the dozens of details involved with assessment and treatment — there is indeed a lot to remember and apply. However, when those tasks have been mastered, we can shift to a broader priority, i.e, “being more focused on the person than on the task” (DiLollo & Favreau, 2010; Granberg & Skagerstrand, 2022; Grosch et al, 2008).
“Being More Focused on the Person Than on the Task”
This short phrase is easy to remember and carries two salient points: (1) being “focused” implicitly includes behaviors typically associated with counseling (active listening, empathy, shared decision-making, etc), and (2) it doesn’t dismiss the importance of our tasks. We can attend to both the person and the tasks in the time allotted, but only if we actively prioritize. When we focus our undivided attention to someone’s personhood for even a very brief time, that person’s experience is about feeling unique, being heard, and sharing responsibility (Feldthusen et al, 2022). Students may not perceive this balance as they master the necessary tasks, but we need to advise them: once these are mastered, move on! Figuring out how to focus more on the person in front of us is our life-long goal.
To the Ida Team…
… Lotte, Ena, Hans, Cher, Natalie, Clint, Anne, Mei and all the change agents at Ida: You brought audiologists together, helped us move forward, and helped persons with hearing loss be heard.
References
Clarke PN, Fawcett J. (2016). Nursing knowledge driving person-centered care. Nursing Science Quarterly, 29(4), 285-287.
DiLollo A, Favreau C. (2010). Person-centered care and speech and language therapy. Seminars in Speech and Language, 31(1), 90-97.
Miles A, Mezzich J. (2011). Person-centered medicine: Advancing methods, promoting implementation. International Journal of Person Centered Medicine, 1(3), 423-428.
 possesses” (1986, p. 391). More simply, “The factors that influence behavior are embedded in the belief that one has the capability to accomplish that behavior” (Klassen & Klassen, 2018, p. 76).
possesses” (1986, p. 391). More simply, “The factors that influence behavior are embedded in the belief that one has the capability to accomplish that behavior” (Klassen & Klassen, 2018, p. 76).



 “Clinician presence” may not be familiar to student trainees, but working with the concept might help them recognize the impact we have on patient impressions and patient outcomes. Clinician presence is defined as a “purposeful practice of awareness, focus, and attention with the intent to understand and connect” (emphasis added) with our patient. Core elements include familiar person/patient-centered behaviors and attributes:2
“Clinician presence” may not be familiar to student trainees, but working with the concept might help them recognize the impact we have on patient impressions and patient outcomes. Clinician presence is defined as a “purposeful practice of awareness, focus, and attention with the intent to understand and connect” (emphasis added) with our patient. Core elements include familiar person/patient-centered behaviors and attributes:2
 patient’s emotions, attitudes, or problems are directly related to living with hearing loss or balance issues; e.g., reactions to diagnosis, concerns about recommendations, or uncertainties about shared decision-making.
patient’s emotions, attitudes, or problems are directly related to living with hearing loss or balance issues; e.g., reactions to diagnosis, concerns about recommendations, or uncertainties about shared decision-making. emotions or behaviors, develops an over-dependence on the clinician, or continues to use offensive language or “overshares”2 after being asked to stop. Clinicians, of course, may also find themselves crossing a boundary, by becoming overly involved with a patient or oversharing about one’s own personal life.
emotions or behaviors, develops an over-dependence on the clinician, or continues to use offensive language or “overshares”2 after being asked to stop. Clinicians, of course, may also find themselves crossing a boundary, by becoming overly involved with a patient or oversharing about one’s own personal life. coordinated healthcare teams. These days, we may likely find ourselves broaching/being broached about topics other than hearing and balance but still relevant to patient health and safety. Audiologists now inquire about medications that may adversely interact with hearing and balance4-7 and are typically required by law to intervene with a referral when we perceive indications of self-harm or suicide ideation.8 Institutions and states require us to report concerns about child and elder abuse.9,10 Other developments include screening for vision problems,11,12 cognitive and memory concerns,13-15 depression,16-19 and childhood bullying20 – of course not to diagnose but to assume responsibility for overall patient health and safety, and direct those concerns to relevant support systems. And although not directly related to our care, of course we will listen and support patients who are coping with a death in the family and similar life experiences. Person-centered care has replaced disease- or disorder-centered care.
coordinated healthcare teams. These days, we may likely find ourselves broaching/being broached about topics other than hearing and balance but still relevant to patient health and safety. Audiologists now inquire about medications that may adversely interact with hearing and balance4-7 and are typically required by law to intervene with a referral when we perceive indications of self-harm or suicide ideation.8 Institutions and states require us to report concerns about child and elder abuse.9,10 Other developments include screening for vision problems,11,12 cognitive and memory concerns,13-15 depression,16-19 and childhood bullying20 – of course not to diagnose but to assume responsibility for overall patient health and safety, and direct those concerns to relevant support systems. And although not directly related to our care, of course we will listen and support patients who are coping with a death in the family and similar life experiences. Person-centered care has replaced disease- or disorder-centered care. Not surprisingly, within a matter of seconds, racial and ethnic minority patients perceive the “unspoken” and understandably distrust the overall situation, including clinical recommendations.6,7 We cannot ignore how this dynamic undermines our goal of providing racially equitable healthcare – indeed, we are obligated to address the problem.
Not surprisingly, within a matter of seconds, racial and ethnic minority patients perceive the “unspoken” and understandably distrust the overall situation, including clinical recommendations.6,7 We cannot ignore how this dynamic undermines our goal of providing racially equitable healthcare – indeed, we are obligated to address the problem. Time to “Reframe”?
Time to “Reframe”?




 human being, that person will likely sense our false front. For example, Apfelbaum et al7 found that Black patients were suspicious of Whites who adopted a colorblind racial perspective, leading them to conclude that a White person who avoids acknowledging race is a racist. Counseling in audiology requires us to communicate with honesty, not cause suspicion and distrust.10,11
human being, that person will likely sense our false front. For example, Apfelbaum et al7 found that Black patients were suspicious of Whites who adopted a colorblind racial perspective, leading them to conclude that a White person who avoids acknowledging race is a racist. Counseling in audiology requires us to communicate with honesty, not cause suspicion and distrust.10,11 3. A Colorblind Stance is Associated with Health Care Disparities
3. A Colorblind Stance is Associated with Health Care Disparities