Samantha Tai, PhD
Lecturer | Audiologist
The University of Melbourne
Victoria, Australia
Over the past couple of years, I’ve been asking our new audiology cohort, ‘What characteristics do you think makes a good audiologist?’ Often, there is a pause before a brave hand will come up to say ‘someone who cares about their patient’, another hand will pop up to say ‘someone knowledgeable, who knows a lot about ears’, another calls out ‘someone who is patient and really listens to the patient’, and then another ‘someone who makes the patient feel comfortable’. While the characteristic of being knowledgeable is often highlighted, the thing that baffles me is students’ intuitive recognition that interpersonal skills are a fundamental characteristic of being a good audiologist. Essentially, it comes down to how we make our patients feel.
In recent years, the scope of practice in the audiology profession has expanded from focusing on a site-of-lesion to a holistic, person-centred approach to hearing care (ASHA, 2018; AudA, 2013; BSA, 2016). That is, the role of an audiologist has moved away from simply being a technician who carries out audiological assessments, to a hearing  professional who empowers and supports patients to self-manage their hearing loss. One of the fundamental elements of patient-centred care is the clinician’s ability to respond to patients’ emotions that have stemmed from their hearing loss. Audiologists who display empathy and acknowledge their patient’s emotions can make their patients feel their concerns are validated and help to reduce psychological distress (Ekberg et al., 2014; Poost-Foroosh et al., 2011). The emphasis on investing in the clinician-patient relationship is beginning to gain recognition in the audiologist’s scope of practice around the world. It falls under the professional guidelines as counselling on the psychosocial impact of the hearing loss (ASHA, 2018; AudA, ACAuD and HAASA, 2016; BSA, 2016).
professional who empowers and supports patients to self-manage their hearing loss. One of the fundamental elements of patient-centred care is the clinician’s ability to respond to patients’ emotions that have stemmed from their hearing loss. Audiologists who display empathy and acknowledge their patient’s emotions can make their patients feel their concerns are validated and help to reduce psychological distress (Ekberg et al., 2014; Poost-Foroosh et al., 2011). The emphasis on investing in the clinician-patient relationship is beginning to gain recognition in the audiologist’s scope of practice around the world. It falls under the professional guidelines as counselling on the psychosocial impact of the hearing loss (ASHA, 2018; AudA, ACAuD and HAASA, 2016; BSA, 2016).
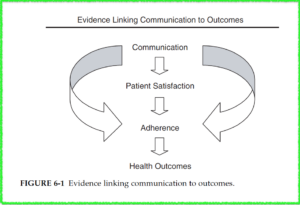
Despite the aforementioned benefits, research has found that when our patients do open up and express their underlying concerns, both experienced clinicians and audiology students tend to miss these opportunities to acknowledge our patients’ emotions (Ekberg et al., 2014; Meyer et al., 2017; Tai et al, 2019). This can have a detrimental effect on the clinician-patient relationship and reduce the likelihood of the patient adhering to recommendations (Ekberg et al., 2014; Grenness et al., 2015). We know that limited acknowledgement or empathetic response is not because of a lack of care or preference for patient-centred care, so it raises the question, why does this deficit exist in our clinical practice?
What are the Current Barriers to Responding to Emotions in Audiology?

Can We Use Our Time Differently?
To put it simply, dealing with emotions is hard and several barriers hinder clinicians to adopt these practices in a clinical setting. To understand some of these barriers, we need to first recognize that traditionally, the audiology profession has placed a significant focus on diagnosing and managing the ‘site-of-lesion’. For instance, in a typical audiological appointment, we invest a majority of time assessing the hearing loss and only a limited time to collate all the relevant questions about the patient’s hearing and thoroughly explain the management options. Similarly, when discussing hearing aid options, audiologists are tasked with convincing the patient that hearing devices are beneficial, give a recommendation, perhaps perform an ear impression, and place an order. With the appointment duration set, clinicians and students alike may find themselves adopting a formulaic approach when communicating with patients, and missing opportunities to address patients’ emotional concerns.
In alignment with the audiology culture, the audiology curriculum was developed to foster students’ diagnostic and technical skills in accordance with the scope of practice. Until recently, counselling skills were absent or minimally integrated into the audiology curricula. Consequently, the lack of formal training means that graduates need to learn counselling skills, including how to respond appropriately to patients’ emotional concerns, on the job. Some clinicians are natural communicators with an innate ability to pick up patient cues and respond empathetically. Honestly, I wouldn’t classify myself as a natural communicator and perhaps there are those of you out there who can relate. I’m sure there are clinicians out there who do not feel comfortable addressing our patient’s emotions because there is
an underlying fear that we might make them feel worse. Without further upskilling or training in counselling skills, experienced clinicians may be unaware of the benefits of acknowledging patient emotions, resulting in the provision of suboptimal hearing care to patients. And through no fault of their own, the missed opportunities to invest in the client-patient relationship may be observed by new graduates or students on clinical placements, who will miss a valuable lesson on how to build a therapeutic relationship.
So What Can We Do to Improve This?
As audiologists, we carry the responsibility to do what’s right by our patients. Although there are things we can’t control such as our educational past or the culture of our workplace, there are plenty of things that are within our control.
Firstly, we need to recognize the way we interact with our patients carries a significant effect on our patient’s hearing outcome. This includes whether they understand their hearing loss, to whether they take your advice about getting an MRI to investigate their asymmetrical hearing loss, or getting and wearing their hearing devices. When we tell our patients they have a hearing loss, we often forget that we’re delivering bad news. On the surface, our patients may be putting on a brave face as they try to listen intently as we describe the circles and crosses on the graph (FYI, sometimes it’s best not to show patients the audiogram). We lose sight that our patients are trying to decipher how their hearing loss will impact their relationships, hobbies, work and perhaps their self-image. If we understand the emotional toll our patients are experiencing due to their hearing loss, then we are more inclined to try and support them through it.
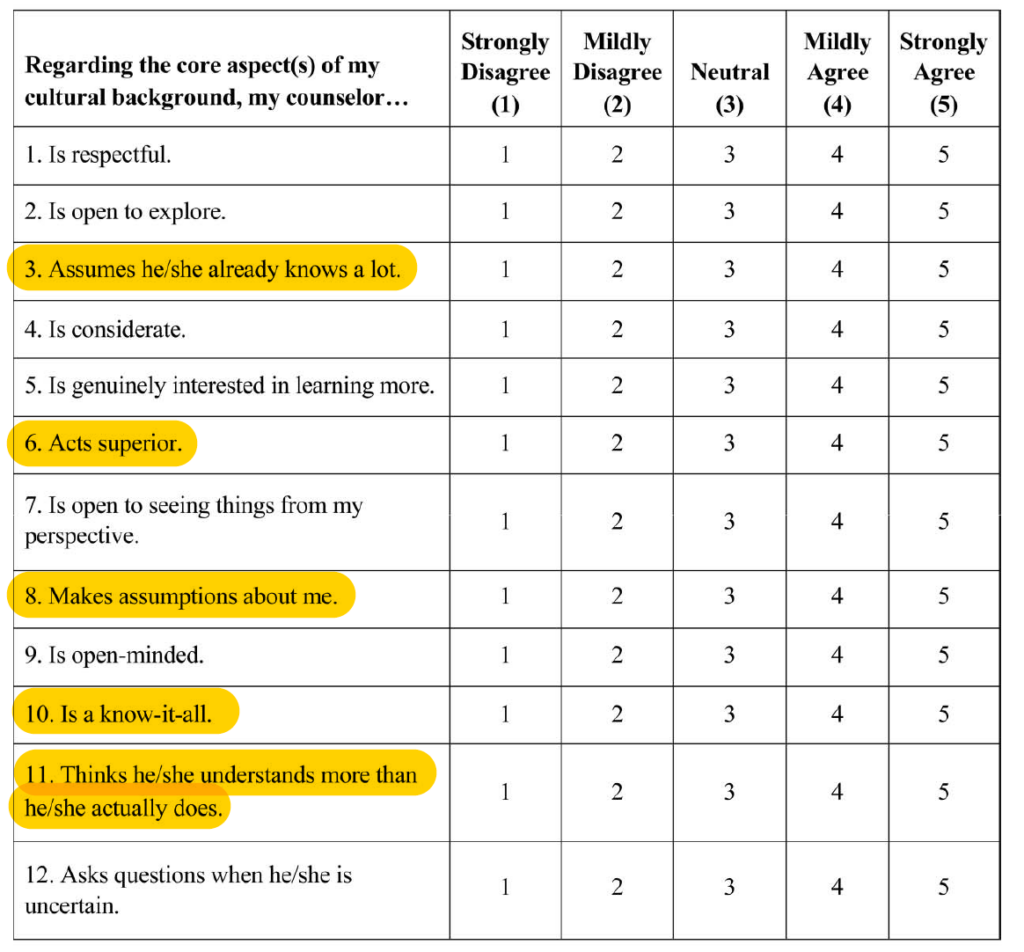
Secondly, we need to critically and honestly examine our own clinical practice and identify any areas that need improvement. In this piece, we’ve focused on acknowledging patient emotions, but it also extends to other areas in our practice. One method is the use of  self-reflective practice where we take a couple of minutes after each appointment to reflect on what went well and what can be improved. Bringing the focus back to addressing patient emotions, we may find that when we recognize and acknowledge our patient’s emotional concerns, he/she starts opening up and we have developed a better rapport. Conversely, we may have noticed a missed opportunity when our patient seemingly joked about early retirement because he can’t carry out his normal work duties. Both scenarios are wonderful opportunities for professional growth and life-long learning.
self-reflective practice where we take a couple of minutes after each appointment to reflect on what went well and what can be improved. Bringing the focus back to addressing patient emotions, we may find that when we recognize and acknowledge our patient’s emotional concerns, he/she starts opening up and we have developed a better rapport. Conversely, we may have noticed a missed opportunity when our patient seemingly joked about early retirement because he can’t carry out his normal work duties. Both scenarios are wonderful opportunities for professional growth and life-long learning.
Finally, we need to invest in ourselves to improve the deficits in our clinical practice. There are many established teaching frameworks available that outlines the key elements of patient-centred communication. For instance, the Calgary Cambridge Guides (Kurtz et al., 1996), or the Four Habits (Krupat et al, 2006) are examples of evidence-based frameworks in medicine that can be translated to an audiological setting. There are also free training resources from the Ida Institute that provides counselling tools for experienced clinicians and students. If other work colleagues are interested in some upskilling, in-house case discussions can include communication strategies to counsel patients in different scenarios. There may even be opportunities for peer learning by observing your colleague’s appointment. Be creative!

References
American Speech-Language-Hearing Association. (2018). Scope of Practice in Audiology. [Accessed October 18, 2018]
AudA, ACAud, & HAASA. (2016). Scope of Practice for Audiologists and Audiometrists, (September), 1-23. [Accessed October 18, 2018]
Audiology Australia. (2013). Professional Practice Standards – Part A Clinical Operations. [Accessed March 29, 2016]
British Society of Audiology. (2016). Practice Guidance: Common Principles of Rehabilitation for Adults in Audiology Services. [Accessed January 17, 2017]
Ekberg, K., Grenness, C., & Hickson, L. (2014). Addressing patients’ psychosocial concerns regarding hearing aids within audiology appointments for older adults. American Journal of Audiology, 23(3), 337–350.
Grenness, C., Hickson, L., Laplante-Lévesque, A., Meyer, C., & Davidson, B. (2015). Communication patterns in audiologic rehabilitation history-taking: Audiologists, patients, and their companions. Ear and Hearing, 36(2), 191–204.
Krupat, E., Frankel, R., Stein, T., & Irish, J. (2006). The Four Habits Coding Scheme: Validation of an instrument to assess clinicians’ communication behavior. Patient Education and Counseling, 62(1), 38-45.
Kurtz, S. M., & Silverman, J. D. (1996). The Calgary-Cambridge Referenced Observation Guides: an aid to defining the curriculum and organizing the teaching in communication training programmes. Medical Education, 30(2), 83–89.
Meyer, C., Barr, C., Khan, A., & Hickson, L. (2017). Audiologist-patient communication profiles in hearing rehabilitation appointments. Patient Education and Counseling, 100(8), 1490–1498.
Poost-Foroosh, L., Jennings, M. B., Shaw, L., Meston, C. N., & Cheesman, M. F. (2011). Factors in client-clinician interaction that influence hearing aid adoption. Trends in Amplification, 15(3), 127–139.
Tai, S., Barr, C., & Woodward-Kron, R. (2019). Towards patient-centred communication: An observational study of supervised audiology student-patient hearing assessments. International Journal of Audiology, 58(2), 97-106.

 Kris English, PhD
Kris English, PhD





 Abi Nardi
Abi Nardi
 We sat down… no one spoke for a minute, we just looked at each other, waiting for the other to speak…when suddenly he said to me: “ How comfortable I have felt for a moment, where nobody told me what to do or how, just waited for me to decide to speak…Now I´m going to tell you…”, Then I asked a few questions, since my patient described himself without questionnaires. And I asked myself: profound hearing loss? Without any testing? It turned out to be a patient with a wrong diagnosis.
We sat down… no one spoke for a minute, we just looked at each other, waiting for the other to speak…when suddenly he said to me: “ How comfortable I have felt for a moment, where nobody told me what to do or how, just waited for me to decide to speak…Now I´m going to tell you…”, Then I asked a few questions, since my patient described himself without questionnaires. And I asked myself: profound hearing loss? Without any testing? It turned out to be a patient with a wrong diagnosis. Luego de saludarnos, nos sentamos… nadie habló por un minuto, solo nos miramos, esperando uno al otro para que hablara… cuando de repente me dijo: “qué a gusto me he sentido por un momento, donde nadie me dijo qué hacer ni cómo, solo me espero a que me decidiera a hablar… Ahora te voy a contar…”, luego realicé pocas preguntas, ya que mi paciente se describió solo sin necesidad de cuestionarios. Y me pregunté: ¿Hipoacusia profunda? Sin haberle realizado siquiera un estudio. Resulto ser un paciente con diagnóstico equivocado desde su narración hasta las pruebas realizadas posteriormente.
Luego de saludarnos, nos sentamos… nadie habló por un minuto, solo nos miramos, esperando uno al otro para que hablara… cuando de repente me dijo: “qué a gusto me he sentido por un momento, donde nadie me dijo qué hacer ni cómo, solo me espero a que me decidiera a hablar… Ahora te voy a contar…”, luego realicé pocas preguntas, ya que mi paciente se describió solo sin necesidad de cuestionarios. Y me pregunté: ¿Hipoacusia profunda? Sin haberle realizado siquiera un estudio. Resulto ser un paciente con diagnóstico equivocado desde su narración hasta las pruebas realizadas posteriormente.
 mind to find peace in the present moment. When we are truly listening, are we also not working to find peace within ourselves to be fully present for the person in front of us?
mind to find peace in the present moment. When we are truly listening, are we also not working to find peace within ourselves to be fully present for the person in front of us? recent being his daughter’s landmark birthday celebration. I let him talk. With tears in his eyes, he told me that he had sought an appointment at his GP for an assessment for dementia. My clinical ego wanted me to reassure him, and tell him everything is fine and to push on with the appointment. But instead, we sat and explored his concerns. We asked each other questions and we sat through conversation and silences that were uncomfortable for the both of us. We came to an agreement that we would get his hearing aids as good as they can be for his dementia assessment, so that we can face things confidently with our heads held high.
recent being his daughter’s landmark birthday celebration. I let him talk. With tears in his eyes, he told me that he had sought an appointment at his GP for an assessment for dementia. My clinical ego wanted me to reassure him, and tell him everything is fine and to push on with the appointment. But instead, we sat and explored his concerns. We asked each other questions and we sat through conversation and silences that were uncomfortable for the both of us. We came to an agreement that we would get his hearing aids as good as they can be for his dementia assessment, so that we can face things confidently with our heads held high.